Overview
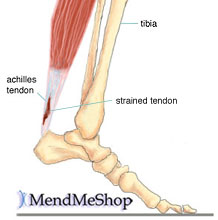
The Achilles tendon is a conjoined tendon composed of the gastrocnemius and soleus muscles with occasional contribution from the plantaris muscle, and it inserts on the calcaneal tuberosity. The plantaris muscle is absent in 6% to 8% of individuals. The Achilles tendon is approximately 15-cm long and is the largest and strongest tendon in the human body. The tendon spirals approximately 90? from its origin to its insertion and this twisting produces an area of stress approximately 2- to 5-cm proximal to its insertion. The tendon has no true synovial sheath; instead it is wrapped in a paratenon. The Achilles tendon experiences the highest loads of any tendon in the body, and bears tensile loads up to 10 times body weight during athletic activities. The tendon most commonly ruptures in a region 2- to 6-cm proximal to its insertion.
Causes
The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop.
Symptoms
When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
The treatments of Achilles tendonitis include resting the painful Achilles tendon will allow the inflammation to subside and allow for healing. A period of rest after the onset of symptoms is important in controlling Achilles tendonitis. In patients who have more significant symptoms, a period of immobilization can help. Either a removable walking boot or a cast can allow the inflamed tendon to cool down quickly. A heel wedge can be inserted into the shoe to minimize the stress on the Achilles tendon. These can be placed in both athletic and work shoes. Applying ice to the area of inflammation can help stimulate blood flow to the area and relieve the pain associated with inflammation. Apply ice several times a day, including after exercise. The pain and swelling most commonly associated with Achilles tendonitis can be improved with non-steroidal, anti-inflammatory medications (NSAIDs) which include Celebrex?, Advil?, Motrin?, Naprosyn?. Be sure to consult your physician before starting any medications. Physical therapists can help formulate a stretching and rehabilitation program to improve flexibility of the Achilles tendon. Cortisone injections should not be used for Achilles tendonitis. Studies have shown an increased incidence of Achilles tendon rupture after cortisone injections.

Surgical Treatment
Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under ?Procedure? in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar.
Prevention
To reduce your chance of developing Achilles tendon problems, follow the following tips. Stretch and strengthen calf muscles. Stretch your calf to the point at which you feel a noticeable pull but not pain. Don't bounce during a stretch. Calf-strengthening exercises can also help the muscle and tendon absorb more force and prevent injury. Vary your exercises. Alternate high-impact sports, such as running, with low-impact sports, such as walking, biking or swimming. Avoid activities that place excessive stress on your Achilles tendons, such as hill running and jumping activities. Choose running surfaces carefully. Avoid or limit running on hard or slippery surfaces. Dress properly for cold-weather training and wear well-fitting athletic shoes with proper cushioning in the heels. Increase training intensity slowly. Achilles tendon injuries commonly occur after abruptly increasing training intensity. Increase the distance, duration and frequency of your training by no more than 10 percent each week.
The Achilles tendon is a conjoined tendon composed of the gastrocnemius and soleus muscles with occasional contribution from the plantaris muscle, and it inserts on the calcaneal tuberosity. The plantaris muscle is absent in 6% to 8% of individuals. The Achilles tendon is approximately 15-cm long and is the largest and strongest tendon in the human body. The tendon spirals approximately 90? from its origin to its insertion and this twisting produces an area of stress approximately 2- to 5-cm proximal to its insertion. The tendon has no true synovial sheath; instead it is wrapped in a paratenon. The Achilles tendon experiences the highest loads of any tendon in the body, and bears tensile loads up to 10 times body weight during athletic activities. The tendon most commonly ruptures in a region 2- to 6-cm proximal to its insertion.
Causes
The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop.
Symptoms
When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
The treatments of Achilles tendonitis include resting the painful Achilles tendon will allow the inflammation to subside and allow for healing. A period of rest after the onset of symptoms is important in controlling Achilles tendonitis. In patients who have more significant symptoms, a period of immobilization can help. Either a removable walking boot or a cast can allow the inflamed tendon to cool down quickly. A heel wedge can be inserted into the shoe to minimize the stress on the Achilles tendon. These can be placed in both athletic and work shoes. Applying ice to the area of inflammation can help stimulate blood flow to the area and relieve the pain associated with inflammation. Apply ice several times a day, including after exercise. The pain and swelling most commonly associated with Achilles tendonitis can be improved with non-steroidal, anti-inflammatory medications (NSAIDs) which include Celebrex?, Advil?, Motrin?, Naprosyn?. Be sure to consult your physician before starting any medications. Physical therapists can help formulate a stretching and rehabilitation program to improve flexibility of the Achilles tendon. Cortisone injections should not be used for Achilles tendonitis. Studies have shown an increased incidence of Achilles tendon rupture after cortisone injections.
Surgical Treatment
Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under ?Procedure? in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar.
Prevention
To reduce your chance of developing Achilles tendon problems, follow the following tips. Stretch and strengthen calf muscles. Stretch your calf to the point at which you feel a noticeable pull but not pain. Don't bounce during a stretch. Calf-strengthening exercises can also help the muscle and tendon absorb more force and prevent injury. Vary your exercises. Alternate high-impact sports, such as running, with low-impact sports, such as walking, biking or swimming. Avoid activities that place excessive stress on your Achilles tendons, such as hill running and jumping activities. Choose running surfaces carefully. Avoid or limit running on hard or slippery surfaces. Dress properly for cold-weather training and wear well-fitting athletic shoes with proper cushioning in the heels. Increase training intensity slowly. Achilles tendon injuries commonly occur after abruptly increasing training intensity. Increase the distance, duration and frequency of your training by no more than 10 percent each week.



 RSS Feed
RSS Feed
